


1.3 Techniques for the head, cervical and upper thoracic spine
![]()
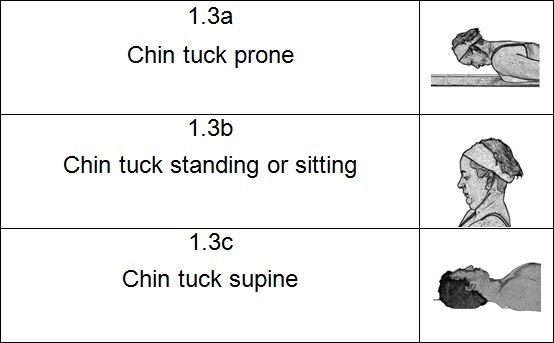
Part A. 1.3 Chin tuck prone
Starting position
- Lay face down on a mat, on the floor or on a table.
- Both arms should rest at the side of the body with your shoulders relaxed.
- Position your head so that you rest on the point of your nose.
Technique
- Take a deep breath in.
- Slowly exhale as you lift your head off the floor.
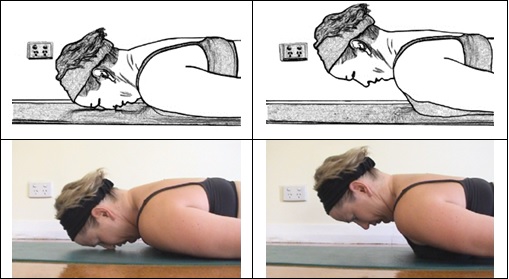
- Careful execution of this technique is necessary for it to be effective.
- As you lift your head keep it parallel with the floor and tuck in your chin.
- Do not tilt your head and neck backwards.
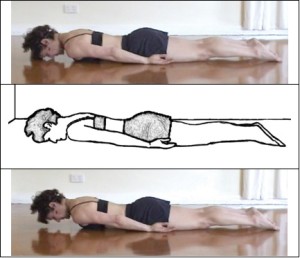
- Your shoulders, ribs and thoracic spine are the foundation that anchors your muscles and enables them to lift your head and neck off the floor.
- Do not lift your chest or lumbar spine off the floor.
- Your shoulders, ribs and mid to lower thoracic spine should not move.
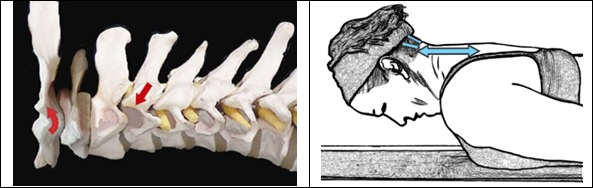
Part B – Direction and range of movement
This technique combines head and neck flexion, with upper and middle thoracic extension. The head and cervical spine translate posteriorly and the head remains parallel with the top-bottom axis of the body at all times.
Total head, cervical and upper thoracic flexion is about 45 degrees. This technique however involves a combination of flexion (nutation) of the occiput, partial cervical flexion and partial upper thoracic extension. Flexion increases from T1 to the occiput and extension increases from T3 to about T6 in the middle of the thoracic spine.
Cervical flexion is neutralised by thoracic extension. Although the head flexes on the atlas and moves (translates) posteriorly, there is no net flexion or extension of the head relative to the spine and the body as a whole. The head remains parallel with the body throughout the technique. At about T2 vertebral level there is a neutral point where there is neither flexion nor extension of the vertebra on the one below.
There should be no extension of the spine below the middle thoracic. In most people the apex of the thoracic kyphosis is at about T6, but the shape of the spine and the apex will vary between individuals.
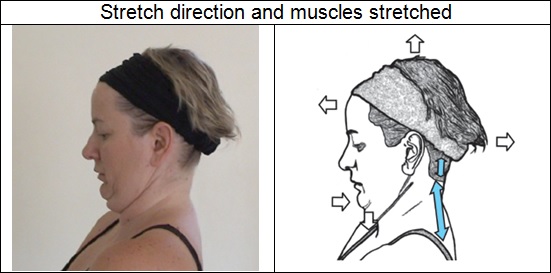
Target tissues
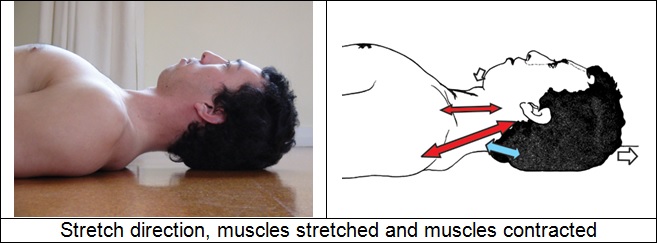
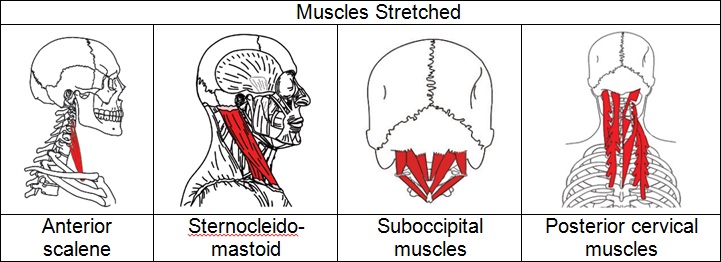
This is an active stretch for the superficial muscles, fascia and ligaments of the posterior cervical and upper thoracic spine and the sub-occipital muscles. The lower origins of these soft tissues are anchored to the posterior part of a vertebra or rib, and the upper ends are attached to the occiput, or another vertebra or rib above. This is also a stretch for sternocleidomastoid and the anterior scalene.
Contraction of the cervical prevertebral muscles produces head and neck flexion. Rectus capitis anterior and longus capitis flex the head, and longus colli flexes the cervical spine.
Contraction of erector spinae and levator scapulae produces posterior translation of the head and neck relative to the rest of the body, lifting the head and neck off the floor when the chin tuck is done prone.
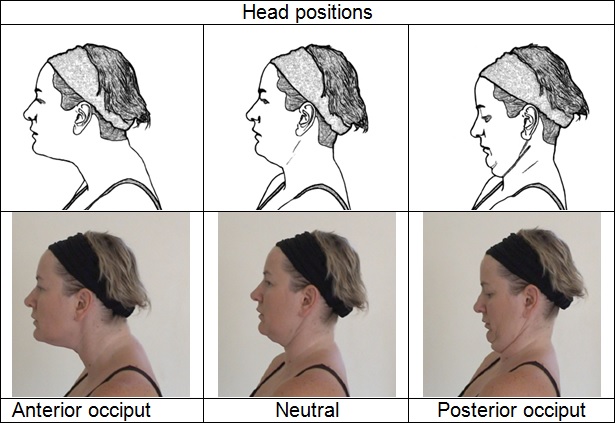
This is a good stretch and a good strengthening exercise. It serves a dual purpose of lengthening short muscles and strengthening key postural muscles, which act against gravity and are subject to postural fatigue. It is a useful technique for correcting common bad posture patterns such as the chin forward posture. In this posture, the occiput is fixed in a bilateral or unilateral anterior position and the cervical spine is fixed in extension.
The anterior occiput is more commonly found on the right side and to correct a right sided anterior occiput it is necessary to introduce head rotation right and sidebending left as you tuck in your chin. The prone chin tuck is the most effective of the chin tuck stretches in strengthening muscles because it requires muscle contraction against gravity.

Safety
If your upper thoracic and cervical spine is very stiff, or if you have an exaggerated thoracic kyphosis or cervical lordosis there may be problems with this technique. When attempting the standing chin tuck you may not be able to touch the wall with the back of your head. When attempting the chin tuck prone you may not be able to lift your head off the floor. When attempting the chin tuck supine you may need a pillow or book under your head to stop your head tilting backwards. After stretching for a while and gaining some flexibility in your upper thoracic spine you may be able to discard the pillow.
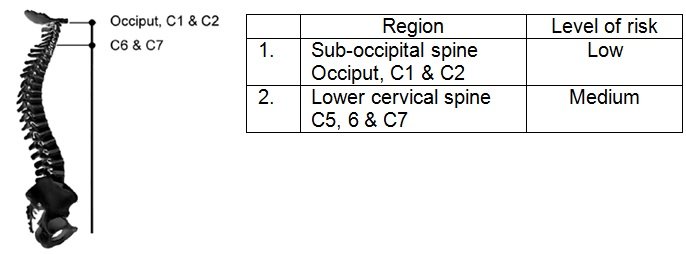
It is important that you do not allow your head to tilt backwards and put strain on your suboccipital spine. Thus ensure you tuck in your chin and keep your head in a vertical plane. Work with your current level of flexibility.
Do not allow movement below the mid thoracic spine. This is more of a problem in the prone chin tuck, where you can more easily lift your shoulder and upper thoracic off the floor. Use a prop to prevent movement – a straight back chair, a wall or the floor. If you do not use a prop then be sure to keep your pelvis upright. When sitting, keep your pelvis perpendicular to the seat and your spine firm, straight and vertical. Keep the stretch localised to the head, neck and upper thoracic spine. The lumbar, lower thoracic spine and pelvis should not move.
If there are degenerative changes in the discs and joints of the lower cervical spine this part of the spine may be sensitive to extension movement and caution may be required when doing this stretch. Use a pillow when attempting the supine chin tuck if there is any degeneration.
Vulnerable areas
Key